Podiatric physicians and surgeons routinely evaluate the osseous structures in their scope when performing diagnosis and treatment. After careful clinical examination where multiple diagnoses are considered, the differential list often leans to radiography for narrowing the diagnosis or confirmation of a diagnosis. Confirmation of osseous healing, whether post-injury or post-operatively (post osteotomy, arthrodesis, etc.), requires visualization of the bone. Likewise, in the study of lower extremity deformities, radiography is indispensable for comprehensive management. Aside from injury and disease states, very often baseline radiographs may be ordered on neuropathic patients, athletes, or in pediatric patients for growth evaluation. These are all reasons why most physicians who routinely treat foot and ankle conditions have in-office X-ray machines.
Podiatric physicians and surgeons routinely evaluate the osseous structures in their scope when performing diagnosis and treatment. After careful clinical examination where multiple diagnoses are considered, the differential list often leans to radiography for narrowing the diagnosis or confirmation of a diagnosis. Confirmation of osseous healing, whether post-injury or post-operatively (post osteotomy, arthrodesis, etc.), requires visualization of the bone. Likewise, in the study of lower extremity deformities, radiography is indispensable for comprehensive management. Aside from injury and disease states, very often baseline radiographs may be ordered on neuropathic patients, athletes, or in pediatric patients for growth evaluation. These are all reasons why most physicians who routinely treat foot and ankle conditions have in-office X-ray machines.
2D vs 3D Imaging
 Standard X-ray generators, along with the developer machines, plumbing, chemicals, and film are not inexpensive. In addition, their usage is somewhat labor intensive, and as with any machine with many moving parts, breakdowns are not infrequent. Quality of image development has inherent inconsistencies with the traditional method and this has arguably been the primary impetus for movement towards digital technology. These newer machines, along with eliminating developer chemicals from the process, have fixed armatures, special image sensors, and software that provides digital contrast enhancement. This combination has removed many of the problematic features of standard radiograph capture and development. While one can easily appreciate the difference in the capture process and quality of these images, one can also appreciate that this technique still has one severe limitation: a 3-dimensional object cannot reliably be reconstructed using a 2-dimensional radiography technique!
Standard X-ray generators, along with the developer machines, plumbing, chemicals, and film are not inexpensive. In addition, their usage is somewhat labor intensive, and as with any machine with many moving parts, breakdowns are not infrequent. Quality of image development has inherent inconsistencies with the traditional method and this has arguably been the primary impetus for movement towards digital technology. These newer machines, along with eliminating developer chemicals from the process, have fixed armatures, special image sensors, and software that provides digital contrast enhancement. This combination has removed many of the problematic features of standard radiograph capture and development. While one can easily appreciate the difference in the capture process and quality of these images, one can also appreciate that this technique still has one severe limitation: a 3-dimensional object cannot reliably be reconstructed using a 2-dimensional radiography technique!

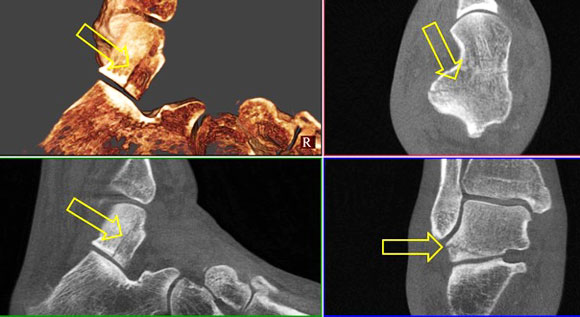
Talar Fracture
Non displaced fracture of the talus. Plain film radiography is limited in visualizing non-displaced fractures as a result of the technique. Length, orientation, and extension of fracture lines into adjacent joints is appreciated in detail with CT. |
|
The Foot and Leg are 3D and Bear Weight
This problem, that traditionally cannot be overcome using ‘plain-film’ radiography, has led to the prescribing of more sophisticated imaging methods. Consequently, ultrasonography (US), magnetic resonance imaging (MRI), and computed tomography (CT) have been a staple in the diagnostic arsenal for decades. It is only recently that the latter method is readily available as an in-office modality for foot and ankle disorders. CT, especially when performed using a weight bearing technique, lends itself readily to hundreds if not thousands of diagnostic dilemmas, deformity scenarios, and study of poly-articular pathology. It is perplexing that a practical 3D imaging modality wasn’t adopted long ago for the lower extremity, a complicated, 3-dimensional, poly-articular structure that has a designated load-bearing kinematic purpose.
Osteochondroma
Osteochondroma as a cause of impingement. On this study the size and location of an exophytic ‘spur’ is appreciated. This is important for both understanding the pathology and for surgical planning. This study reveals that the spur is extraarticular and over the medial talar neck, so surgical approach is carried out appropriately. |
|
An Enormous Potential to Improve Podiatric Diagnosis
A staple modality in foot and ankle fracture evaluation (e.g., Lisfranc fracture/dislocations, calcaneal and pilon fractures), CT has now advanced in the evaluation of kinematics, made possible by load bearing. This dramatically extends the indications for studies where kinematics leads to pathology. For example, medial column instability can now be more fully understood, as can talo-tarsal and subtarsal subluxation, intercuneiform instability, and cuboid syndrome. Hallux limitus, one of the more compelling conditions due to its ubiquitous nature as an apex pathology (more proximal pathology often results) can now be fully understood radiographically leading to more accurate diagnosis and treatment – likewise for almost any arthrosis. Osteochondroses are not only more accurately defined for size and position, but also for their extent of contribution to joint pathology in the presence of multi-focal articular disease. Deformity after fracture healing is better appreciated specifically as it relates to weight-bearing conditions. Fractures, whether acute (e.g., sesamoid or metatarsal) or chronic (non-unions) of weight bearing bones can be understood better, as they will demonstrate measurable displacement under load, which will guide treatment more accurately. Evaluation of the infra- and posterior calcaneal spur are better understood in their anatomic structure, alignment or displacement using CT. Osteomyelitis and infectious osteitis are better managed using this modality over conventional radiographs, especially when evaluating for bone resection that may change the weight-bearing pattern (parabola in the forefoot) or midfoot. The list goes on, and every foot and ankle surgeon could probably think of hundreds of other conditions for which weight-bearing CT, if immediately available to them, would enhance their diagnostic capabilities.

Tarsal Coalition
Tarsal coalition. This patient presented with peroneal spasm, rigid flatfoot, and dorsal talonavicular beak; MRI elsewhere related no obvious coalition. This series demonstrates the coalition readily and adjacent joint degeneration. Studies like this are an essential part of preoperative planning. |
|
But at What Price?
Technology in medicine, of course, comes at a price to all who are involved: doctors, insurers, and the patients. Substantial expensive research and development was required to bring these sophisticated tools to us, but along with sophisticated tools come better diagnostic capabilities and consequently better care. The price of a wrong diagnosis, or a partial diagnosis, is far more expensive over the long run than accurate assessment the first time around. This is where the science of medicine is critical, and is why we invest in ourselves and our practices as physicians and surgeons – we know how valuable it is to make the correct diagnosis based on all the information that can be obtained. However, it makes sense to look at the complete financial picture of using in-office CT in a real-world practice environment.
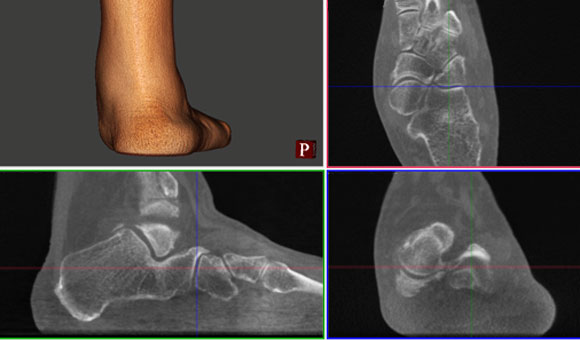
Pes valgus
Pes valgus with polyarticular degeneration. Here the subtalar joint pathology is readily appreciated, as is the resultant medial column degeneration, from the hindfoot to the first metatarsophalangeal joint. Weight bearing produces the most detailed view of the joint kinematics that leads to polyarticular disease. |
|
You